In 1983 the loss of life on Air Canada 797 changed the way we pilots prioritize cabin fires. We moved from "fight the fire first, land if you have to," to "point the aircraft to a runway, fight the fire if you can." The incident also prompted changes to the way aircraft interiors are built. See Air Canada 797. Fifteen years later, the case of Swissair 111 served new lessons in pilot procedures and cabin electronics.
— James Albright
Updated:
2020-09-18

Swiss Air HB-IWF
Swissair 111 was en route from New York to Geneva when a power cable to the cabin inflight entertainment system arced and caused smoke and fire in cabin insulation near the cockpit. The crew incorrectly assumed it was an air conditioning smell, but made an early, and correct, decision to divert the aircraft. They failed, however, to aggressively fight the fire and expedite their descent. In fact, they deliberately slowed their descent to provide more time to prepare the cabin for landing and later requested a turn away from the airport to dump fuel. During that turn away the fire spread and intensified, degrading aircraft systems and primary cockpit displays. All on board perished.
The Transportation Safety Board of Canada cuts the crew a great deal of slack, saying that even had they not made these two delaying actions, the fire would have left the airplane unflyable short of their divert airport. I'm not so sure. Looking at the flight profile map, shown above, I think an aggressive descent and willingness to land the airplane overweight would have damaged the aircraft, to be sure, but would have saved many lives. That is not to say I blame the crew, they were acting as many of us would have in 1998. We need to take away from this mishap two very important lessons:
- If you have a cabin fire, your first decision must be to point the airplane to a landable surface, preferably a long runway with fire coverage. You need to fly fast, the clock is ticking.
- If you have a cabin crew, they must fight the fire aggressively.
We now know that statistics show if you don't put out a cabin fire in eight minutes or less, it will probably become uncontrollable. We also know that if you have an uncontrollable cabin fire you probably have only fifteen minutes before the fire renders the airplane unflyable. More about this: Cabin Fire.
1
Accident report
- Date: 02 SEP 1998
- Time: 21:31
- Type: McDonnell Douglas MD-11
- Operator: Swissair
- Registration: HB-IWF
- Fatalities: 14 of 14 crew, 229 of 229 passengers
- Aircraft Fate: Destroyed
- Phase: En route
- Departure Airport: New York-John F. Kennedy International Airport, NY (JFK/KJFK), United States of America
- Destination Airport: Genève-Cointrin Airport (GVA/LSGG), Switzerland
2
Narrative
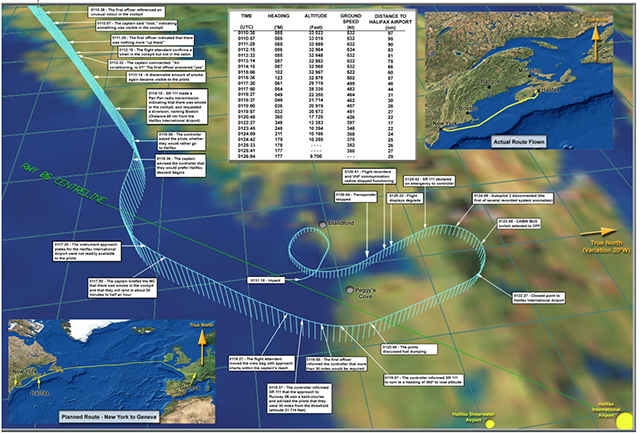
Flight profile, AIB, Appendix IX-A
- At 0018 UTC (2018 eastern daylight savings time) on 2 September 1998, the McDonnell Douglas (MD) MD-11, operating as SR 111, departed John F. Kennedy (JFK) International Airport in Jamaica, New York, United States of America (USA), on a flight to Geneva, Switzerland. Two pilots, 12 flight attendants, and 215 passengers were on board. The first officer was the pilot flying. At 0058, SR 111 contacted Moncton Air Traffic Services (ATS) Area Control Centre (ACC) and reported that they were at flight level (FL) 330.
- At 0110:38, the pilots detected an unusual odour in the cockpit and began to investigate. They determined that some smoke was present in the cockpit, but not in the passenger cabin. They assessed that the odour and smoke were related to the air conditioning system. At 0114:15, SR 111 made a Pan Pan radio transmission to Moncton ACC. The aircraft was about 66 nautical miles (nm) southwest of Halifax International Airport, Nova Scotia. The pilots reported that there was smoke in the cockpit and requested an immediate return to a convenient place. The pilots named Boston, Massachusetts, which was about 300 nm behind them. The Moncton ACC controller immediately cleared SR 111 to turn right toward Boston and to descend to FL 310. At 0115:06, the controller asked SR 111 whether they preferred to go to Halifax, Nova Scotia. The pilots expressed a preference for Halifax, which was considerably closer. They immediately received an ATS clearance to fly directly to Halifax, which was by then about 56 nm to the northeast. At this time, the pilots donned their oxygen masks.
- At 0116:34, the controller cleared SR 111 to descend to 10 000 feet above sea level, and asked for the number of passengers and amount of fuel on board. The pilots asked the controller to stand by for that information. At 0118:17, the controller instructed SR 111 to contact Moncton ACC on radio frequency (RF) 119.2 megahertz (MHz). SR 111 immediately made contact with Moncton ACC on 119.2 MHz and stated that the aircraft was descending out of FL 254 on a heading of 050 degrees6 on course to Halifax. The controller cleared SR 111 to 3 000 feet. The pilots requested an intermediate altitude of 8 000 feet until the cabin was ready for landing.
- At 0119:28, the controller instructed SR 111 to turn left to a heading of 030 for a landing on Runway 06 at the Halifax International Airport, and advised that the aircraft was 30 nm from the runway threshold. The aircraft was descending through approximately FL 210 and the pilots indicated that they needed more than 30 nm. The controller instructed SR 111 to turn to a heading of 360 to provide more track distance for the aircraft to lose altitude. At 0120:48, the flight crew discussed internally the dumping of fuel based on the aircraft's gross weight, and on their perception of the cues regarding the aircraft condition, and agreed to dump fuel. At 0121:20, the controller made a second request for the number of persons and amount of fuel on board. SR 111 did not relay the number of persons on board, but indicated that the aircraft had 230 tonnes (t) of fuel on board (this was actually the current weight of the aircraft, not the amount of fuel) and specified the need to dump some fuel prior to landing.
- At 0121:38, the controller asked the pilots whether they would be able to turn to the south to dump fuel, or whether they wished to stay closer to the airport. Upon receiving confirmation from the pilots that a turn to the south was acceptable, the controller instructed SR 111 to turn left to a heading of 200, and asked the pilots to advise when they were ready to dump fuel. The controller indicated that SR 111 had 10 nm to go before it would be off the coast, and that the aircraft was still within 25 nm of the Halifax airport. The pilots indicated that they were turning and that they were descending to 10 000 feet for the fuel dumping.
- At 0122:33, the controller heard, but did not understand, a radio transmission from SR 111 that was spoken in Swiss–German, and asked SR 111 to repeat the transmission. The pilots indicated that the radio transmission was meant to be an internal communication only; the transmission had referred to the Air Conditioning Smoke checklist.
- At 0123:30, the controller instructed SR 111 to turn the aircraft farther left to a heading of 180, and informed the pilots that they would be off the coast in about 15 nm. The pilots acknowledged the new heading and advised that the aircraft was level at 10 000 feet.
- At 0123:53, the controller notified SR 111 that the aircraft would be remaining within about 35 to 40 nm of the airport in case they needed to get to the airport in a hurry. The pilots indicated that this was fine and asked to be notified when they could start dumping fuel. Twenty seconds later, the pilots notified the controller that they had to fly the aircraft manually and asked for a clearance to fly between 11,000 and 9 000 feet. The controller notified SR 111 that they were cleared to fly at any altitude between 5 000 and 12 000 feet.
- At 0124:42, both pilots almost simultaneously declared an emergency on frequency 119.2 MHz; the controller acknowledged this transmission. At 0124:53, SR 111 indicated that they were starting to dump fuel and that they had to land immediately. The controller indicated that he would get back to them in just a couple of miles. SR 111 acknowledged this transmission.
- At 0125:02, SR 111 again declared an emergency, which the controller acknowledged. At 0125:16, the controller cleared SR 111 to dump fuel; there was no response from the pilots. At 0125:40, the controller repeated the clearance. There was no further communication between SR 111 and the controller.
- At approximately 0130, observers in the area of St. Margaret's Bay, Nova Scotia, saw a large aircraft fly overhead at low altitude and heard the sound of its engines. At about 0131, several observers heard a sound described as a loud clap. Seismographic recorders in Halifax, Nova Scotia, and in Moncton, New Brunswick, recorded a seismic event at 0131:18, which coincides with the time the aircraft struck the water. The aircraft was destroyed by impact forces. There were no survivors.
Source: Aviation Investigation Report, ¶1.1
3
Analysis
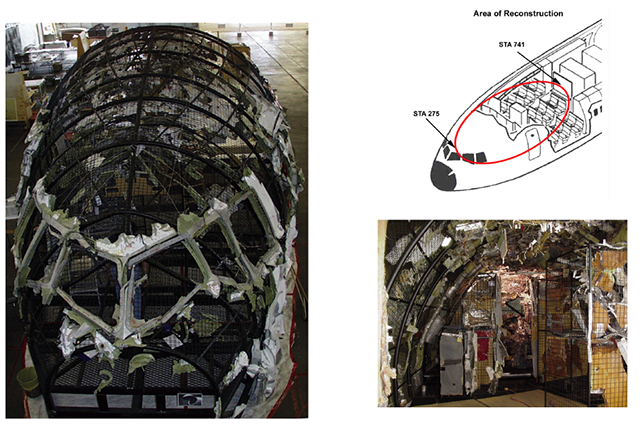
Reconstruction, AIB
The crew did a lot right but their training let them down. We pilots do not judge smells correctly and they mistakenly thought their problem was in the air conditioning system and the situation wasn't as dire as it really was. They placed a higher priority on running checklists, allowing the cabin crew to prepare the aircraft for landing, and not dumping fuel over land than they did on getting their aircraft on the ground expeditiously. I think it fair to say most pilots had similar views in 1998. The following timeline, extracted from the report, should serve to show why "speed is life" when dealing with a cabin fire:
| UTC Time | Elapsed Time (minutes) | Event |
| 0110:38 | 00:00 | Unusual smell detected in the cockpit |
| 0115:36 | 04:58 | Decision made to divert to Halifax, Nova Scotia |
| 0115:56 | 05:18 | The captain donned his oxygen mask |
| 0116:03 | 06:25 | The first officer donned his oxygen mask |
| 0117:38 | 07:00 | The captain indicated to the first officer that he should not descend too fast |
| 0119:37 | 08:59 | The controller advised the flight crew that they were 30 miles from the threshold of Runway 06 |
| 0119:50 | 09:12 | The first officer informed the controller that more than 30 miles would be required. |
| 0120:54 | 10:16 | Decision made to dump fuel |
| 0121:46 | 11:08 | The pilots decided that turning to the south for fuel dumping would be appropriate. (The controller gave them a choice of turning south or staying closer to the airport.) |
| 0123:45 | 13:07 | CABIN BUS switch selected to OFF |
| 0124:42 | 14:04 | Emergency declared |
| 0125:41 | 15:03 | Recorders stop recording. (The flight data recorder noted a cascading list of failure from both yaw dampers to flight instruments.) |
| 0131:18 | 15:03 | Impact with water |
4
Cause
- Aircraft certification standards for material flammability were inadequate in that they allowed the use of materials that could be ignited and sustain or propagate fire. Consequently, flammable material propagated a fire that started above the ceiling on the right side of the cockpit near the cockpit rear wall. The fire spread and intensified rapidly to the extent that it degraded aircraft systems and the cockpit environment, and ultimately led to the loss of control of the aircraft.
- Metallized polyethylene terephthalate (MPET)-type cover material on the thermal acoustic insulation blankets used in the aircraft was flammable. The cover material was most likely the first material to ignite, and constituted the largest portion of the combustible materials that contributed to the propagation and intensity of the fire.
- Once ignited, other types of thermal acoustic insulation cover materials exhibit flame propagation characteristics similar to MPET-covered insulation blankets and do not meet the proposed revised flammability test criteria. Metallized polyvinyl fluoride–type cover material was installed in HB-IWF and was involved in the in-flight fire.
- Silicone elastomeric end caps, hook-and-loop fasteners, foams, adhesives, and thermal acoustic insulation splicing tapes contributed to the propagation and intensity of the fire.
- The type of circuit breakers (CB) used in the aircraft were similar to those in general aircraft use, and were not capable of protecting against all types of wire arcing events. The fire most likely started from a wire arcing event.
- A segment of in-flight entertainment network (IFEN) power supply unit cable (1-3791) exhibited a region of resolidified copper on one wire that was caused by an arcing event. This resolidified copper was determined to be located near manufacturing station 383, in the area where the fire most likely originated. This arc was likely associated with the fire initiation event; however, it could not be determined whether this arced wire was the lead event.
- There were no built-in smoke and fire detection and suppression devices in the area where the fire started and propagated, nor were they required by regulation. The lack of such devices delayed the identification of the existence of the fire, and allowed the fire to propagate unchecked until it became uncontrollable.
- There was a reliance on sight and smell to detect and differentiate between odor or smoke from different potential sources. This reliance resulted in the misidentification of the initial odor and smoke as originating from an air conditioning source.
- There was no integrated in-flight fire fighting plan in place for the accident aircraft, nor was such a plan required by regulation. Therefore, the aircraft crew did not have procedures or training directing them to aggressively attempt to locate and eliminate the source of the smoke, and to expedite their preparations for a possible emergency landing. In the absence of such a fire fighting plan, they concentrated on preparing the aircraft for the diversion and landing.
- There is no requirement that a fire-induced failure be considered when completing the system safety analysis required for certification. The fire-related failure of silicone elastomeric end caps installed on air conditioning ducts resulted in the addition of a continuous supply of conditioned air that contributed to the propagation and intensity of the fire.
- The loss of primary flight displays and lack of outside visual references forced the pilots to be reliant on the standby instruments for at least some portion of the last minutes of the flight. In the deteriorating cockpit environment, the positioning and small size of these instruments would have made it difficult for the pilots to transition to their use, and to continue to maintain the proper spatial orientation of the aircraft.
Source: Aviation Investigation Report, ¶3.1
References
(Source material)
Mayday: Fire on Board, Cineflix, Episode 3, Season 1, 22 October 2003 (Swissair 111)
Transportation Safety Board of Canada, Aviation Investigation Report, A98H0003, In-flight Fire Leading to Collision with Water, Swissair Transport Limited, McDonnell Douglas MD-11 HB-IWF, Peggy's Cove, Nova Scotia 4 nm SW, 2 September 1998