The NTSB Report does a good job of relaying the events of Flight 797 but perhaps fails to emphasize a few key points.
— James Albright
Updated:
2014-05-26

Airplane after fire burned through,
from NTSB Report, Figure 2.
The captain attempted a second reset of three popped circuit breakers even after noting he felt them pop as he pushed them. As it turns out, the resetting of the circuit breakers did not cause the fire, but the danger posed bears discussion:
- In 1983, Air Canada policy allowed crews to reset circuit breakers multiple times if they were allowed to cool "about 3 minutes." I was flying an Air Force Boeing 707 at the time and its manual was about the same: [Technical Order 1C-135(E)C-1, pg. 1-57] "Circuit breakers may be pulled and reset without damage to the circuit breaker; however, circuit breaker pulling should be kept to a minimum."
- These days most manuals are more like what appears in the G450 Aircraft Flight Manual, pg. 4 - 1] "Resetting "tripped" circuit breakers or cycling circuit breakers to recover or "re-boot" systems should be done only if the system is required for continued safe flight and landing."
The captain delayed the decision to land for six minutes after first being told there was a fire, in the hope that the fire would go out. It could very well be that had he decided to land immediately the results would have been very different.
- The airplane was airborne for nearly 20 minutes after the captain was first informed there was a fire. The industry has had a philosophy change on fire and smoke and fumes elimination. Before it was fight the fire, land if you must. Now it is land as soon as possible, fight the fire if you can.
- Had the decision been made earlier, many of the further complicating factors (electrical failures, ATC mishandled vectors, evacuation confusion because of smoke) would not have happened.
- As a result of this mishap, the industry now mandates better fire warning systems, fire retardant interiors, and procedural changes to make help get the airplane headed toward landing sooner and to improve evacuation procedures.
I don't offer these critiques in an effort to point fingers, only to drive home this point: if you don't put the fire out in eight minutes you won't be able to and if you don't get the airplane on the ground in fifteen minutes you won't be landing on your own terms. When in doubt, land. More about this: Cabin Fire.
1
Accident report
- Date: 02 JUN 1983
- Time: 19:20
- Type: McDonnell Douglas DC-9-32
- Operator: Air Canada
- Registration: C-FTLU
- Fatalities: 0 of 5 crew, 23 of 46 passengers
- Aircraft Fate: Destroyed
- Phase: En route
- Airports: (Departure) Dallas/Fort Worth International Airport, TX (DFW/KDFW), United States of America (Destination) Toronto International Airport, ON (YYZ/CYYZ), Canada
2
Narrative
- On June 2, 1983, Air Canada Flight 797, a McDonnell Douglas DC-9-32, of Canadian Registry C-FTLU, was a regularly scheduled international passenger flight from from Dallas, Texas to Montreal, Quebec, Canada, with an en route stop at Toronto, Ontario, Canada. The flight left Dallas with 5 crewmembers and 41 passengers on board.
Source: NTSB Aircraft Accident Report, AAR-86/02, page 1
- At 1851:14 eastern daylight time, the three circuit breakers associated with the aft lavatory's flush motor and located on a panel on the cockpit wall behind the captain's seat, tripped in rapid succession. (The motor is a three-phase alternating current (a.c.) motor; each phase incorporates a circuit breaker for protective purposes.) After identifying the circuit breakers, the captain immediately made one attempt to reset them; the circuit breakers would not reset. The captain assumed that the flush motor had probably seized and took no further action at this time. About 1859:58, the captain again tried unsuccessfully to reset the three circuit breakers. According to the cockpit voice recorder (CVR), he told the first officer that the circuit breaker(s), "Pops as I push it."
Source: NTSB Aircraft Accident Report, AAR-86/02, page 2
This was accepted practice at the time, we know better now. Pilot's should also understand that a component on three phases of AC current are very high draw items.
See: Three Phase Electrical Power.
- About 1900, a passenger seated in the last row asked the No. 3 flight attendant to identify a strange odor. The flight attendant thought the odor was coming from the aft lavatory. She took a CO2 fire extinguisher from the cabin wall and opened the lavatory door a few inches. She saw that a light gray smoke had filled the lavatory from the floor to the ceiling, but she saw no flames. While she was inspecting the lavatory, she inhaled some smoke and closed the door. The No. 3 flight attendant then saw the No. 2 flight attendant nearby and asked her to tell the flight attendant in charge of the situation. The No. 2 flight attendant testified that she did not remember if she had been told there was smoke or fire in the lavatory; however, when she reached the flight attendant in charge she told him there was a fire in the lavatory.
- Upon being advised there was a fire, the flight attendant in charge instructed the No. 2 flight attendant to inform the captain and then to assist the No. 3 flight attendant in moving the passengers forward and in opening the eyebrow air vents over the passenger seats to direct air to the rear of the cabin.
Source: NTSB Aircraft Accident Report, AAR-86/02, page 2
It seems this was a common thought process back then in most airlines, deal with the problem and continue to your destination. I had a cabin fire in an Air Force airplane the same year and our reaction was the put the airplane on the ground as soon as possible.
Most of the aviation world is on board with this philosophy now, as detailed in Advisory Circular 120-80.
- At 1902:40, the No. 2 flight attendant reached the cockpit and told the captain, "Excuse me, there's a fire in the washroom in back, they're just . . . went back to go to put it out." Upon being notified of the fire, the captain ordered the first officer to inspect the lavatory. The captain then donned his oxygen mask and selected the 100-percent oxygen position of his regulator.
- At 19:04:07, the first officer returned to the cockpit and told the captain that the smoke had prevented him from entering the aft lavatory and that he thought "we'd better go down."
- [The first officer returned to the cockpit for a set of smoke goggles, After he retrieved them the captain directed him to go aft again.]
- At 1906:52, while the first officer was out of the cockpit, the flight attendant in charge told the captain again that the smoke was clearing. The captain testified that he believed the fire was in the lavatory trash bin and that he did not decide to descend at this time because, "I expected it (the fire) to be put out."
Source: NTSB Aircraft Accident Report, AAR-86/02, page 2
Nobody mentioned a trash bin fire, he should have connected the dots between the three popped circuit breakers and the fire.
- About 1905:35, while the first officer was aft to inspect the aft lavatory, the airplane had experienced a series of electrical malfunctions. According to the captain, the master caution light illuminated, indicating that the airplane's left a.c. and d.c. electrical systems had lost power. At 1906:12, the captain called Indianapolis Center and requested the Center to standby because the flight had an "electrical problem."
Source: NTSB Aircraft Accident Report, AAR-86/02, page 2
He should have realized he had more than an electrical problem.
- At 19:08:12, Flight 797 called the radar high sector controller at Indianapolis Center and said, "Mayday, Mayday, Mayday." The Louisville radar high sector controller acknowledged to call, and at 1908:47, the flight told the controller that it had a fire and was going down.
- The captain began the emergency descent almost simultaneously with the "Mayday" call. The throttles were retarded to idle and the speed brakes were extended.
- The descent was flown at 310 knots indicated airspeed (KIAS), and since the needle on the instantaneous vertical speed indicator (IVSI) was pegged, the rate of descent exceeded 6,000 feet per minute (fpm).
Source: NTSB Aircraft Accident Report, AAR-86/02, page 2
The aircraft's transponder was among the systems lost and air traffic control had difficulty painting the aircraft and providing the most expeditious descent vectors. It wasn't until 19:14:03 that the approach controller was able to fully identify the flight. This didn't particularly delay the descent, but it created confusion on the ground as to where the fire trucks should be positioned.
- At 1920:09, the local controller told the approach controller, "He's landed."
Source: NTSB Aircraft Accident Report, AAR-86/02, page 2
3
Analysis
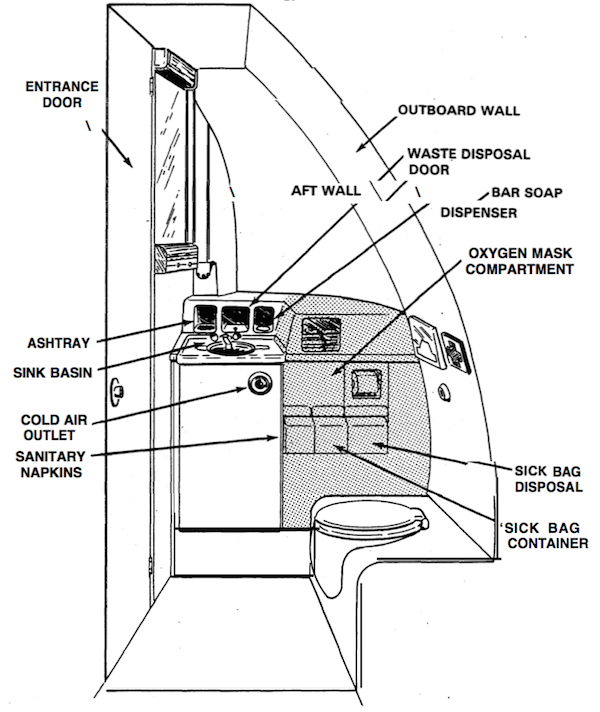
Diagram of aft lavatory, from NTSB Report, Figure 9.
- The evidence substantiates a conclusion that when the smoke was detected by the flight attendants, there was a fire located within the vanity and/or the toilet shroud in the lavatory.
Source: NTSB Aircraft Accident Report, AAR-86/02, ¶2.2
Investigators ruled out the trash bin itself as a source of the fire but could not rule out the possibility that there was debris behind the bin and that a lit cigarette could have fallen in that space. They further concluded it was "unlikely that the flush motor was the source of ignition of the fire." They also concluded the flush motor wiring harness was unlikely to be the cause. The investigated the possibility of a generator feeder cable nearby could have shorted, while they had no evidence supporting this, the possibility "could not be dismissed."
4
Cause
- Since the fire was already well established, the attempts to reset the circuit breakers had no effect on the sequence of events.
Source: NTSB Aircraft Accident Report, AAR-86/02, ¶2.3
- A fire propagated through the amenities section of the aft lavatory and had burned undetected for almost 15 minutes before the smoke was first detected.
- The Safety Board count not identify the origin of the fire.
- The first malfunction to evidence itself to the flightcrew was the simultaneous tripping of the three flush motor circuit breakers, about 11 minutes before the smoke was discovered. The flightcrew did not consider this to be a serious problem.
- The source of the smoke was never identified either by the flight attendant of the first officer. The captain was never told nor did he inquire as the precise location and extent of the "fire," which had been reported to him. Crewmember reports that the first was abating misled the captain about the severity and he delayed his decision to declare an emergency and descend.
- Because of the delayed decision to descend, the airplane lost the opportunity to be landed at Louisville. Had the airplane had been landed at Louisville, it could have been landed 3 to 5 minutes earlier than it actually did land at Cincinnati. The delayed decision to descend and land contributed to the severity of the accident.
Source: NTSB Aircraft Accident Report, AAR-86/02, ¶3.1
- The National Transportation Safety Board determines that the probable causes of the accident were a fire of undetermined origin, an underestimate of fire severity, and conflicting fire progress information provided to the captain.
Source: NTSB Aircraft Accident Report, AAR-86/02, ¶3.2
There is an art to reading an accident report, especially one that involves more than one country and several companies that could be found liable. If you want to see what the real cause of an accident is, look at the recommendations. The purpose of the investigation, after all, is to prevent recurrence. From a pilot perspective we need to learn the lesson: "land the airplane as soon as possible, fight the fire if time permits." But what really caused the fire and what has been done to keep this from happening again?
- The Safety Board recommended on July 19, 1983, that the FAA: Issue an Airworthiness Directive (1) to require an immediate inspection of the lavatory flushing pump motor and the associated wiring harnesses between the timing components and the motor in the lavatories of transport category airplanes for evidence of moisture-induced corrosion or deteriorated insulation and to require that flushing pump motors or wiring harnesses which exhibit such conditions be replaced, and (2) to establish appropriate periodic intervals for repetition of these inspections.
Source: NTSB Aircraft Accident Report, AAR-86/02, §4
References
(Source material)
Advisory Circular 120-80, In-flight Fires, 1/8/04, U.S. Department of Transportation
Gulfstream G450 Airplane Flight Manual, Revision 35, April 18, 2013
NTSB Aircraft Accident Report, AAR-86/02, Air Canada Flight 797 McDonnell Douglas DC-9-32, C-FTLU Greater Cincinnati International Airport Covington, Kentucky, June 2, 1983
Technical Order 1C-135(E)C-1, EC-135C Flight Manual, USAF Series, 15 February 1966