I think it is a sad story whenever a perfectly good airplane is flown into the ground, but this one more so because it was a suicide. As heartless as it may seem, we should be classifying it as a case of involuntary manslaughter because innocent lives were taken as well. Are there lessons here for us pilots. Yes, indeed.
— James Albright
Updated:
2018-10-02

General view of the accident site,
Final Report, Figure 12.
I think the lesson here is that we pilots have to take care of ourselves both mentally and physically, and just as importantly, we need to keep an eye on our fellow pilots.
1
Accident report
- Date: 24 March 2015
- Time: 10:41
- Type: Airbus A320-211
- Operator: Germanwings
- Registration: D-AIPX
- Fatalities: 6 of 6 crew, 150 of 150 passengers
- Aircraft fate: Destroyed
- Phase: En route
- Airport (departure): Barcelona-El Prat Airport (LEBL)
- Airport (arrival): Düseldorf International Airport (EDDL)
2
Narrative
- The takeoff from Barcelona took place at 9 h 00 from runway 07R. The co-pilot was Pilot Flying (PF).
- At 9 h 30 min 08, the Captain told the co-pilot that he was leaving the cockpit and asked him to take over radio communications, which the co-pilot acknowledged.
- At 9 h 30 min 24, noises of the opening then, three seconds later, the closing of the cockpit door were recorded. The Captain was then out of the cockpit.
- At 9 h 30 min 53, the selected altitude on the FCU changed in one second from 38,000 ft to 100 ft. One second later, the autopilot changed to OPEN DES mode and autothrust changed to THR IDLE mode. The aeroplane started to descend and both engines’ speed decreased.
Source: Final Report, ¶1.1
The OPEN DESCENT mode of the autopilot manages aircraft pitch to maintain a target speed while the auto thrust, if engaged, commands idle.
- At 9 h 33 min 12, the speed management changed from managed mode to selected mode. One second later, the selected target speed became 308 kt while the aeroplane’s speed was 273 kt. The aeroplane’s speed started to increase along with the aeroplane’s descent rate, which subsequently varied between 1,700 ft/min and 5,000 ft/min, then was on average about 3,500 ft/min.
- At 9 h 33 min 35, the selected speed decreased to 288 kt. Then, over the following 13 seconds, the value of this target speed changed six times until it reached 302 kt.
- At 9 h 33 min 47, the controller asked the flight crew what cruise level they were cleared for. The aeroplane was then at an altitude of 30,000 ft in descent. There was no answer from the co-pilot. Over the following 30 seconds, the controller tried to contact the flight crew again on two occasions, without any answer.
- At 9 h 34 min 23, the selected speed increased up to 323 kt. The aeroplane’s speed was then 301 kt and started to increase towards the new target.
- At 9 h 34 min 31, the buzzer to request access to the cockpit was recorded for one second.
- At 9 h 34 min 38, the controller again tried to contact the flight crew, without any answer.
- At 9 h 34 min 47 then at 9 h 35 min 01, the Marseille control centre tried to contact the flight crew on 133.330 MHz, without any answer. The aeroplane was then at an altitude of 25,100 ft, in descent.
- At 9 h 35 min 03, the selected speed increased again to 350 kt.
- Subsequently, and until the end of the recording:
- the selected speed remained at 350 kt and the aeroplane’s speed stabilised around 345 kt;
- the autopilot and autothrust remained engaged;
- the cockpit call signal from the cabin, known as the cabin call, from the cabin interphone, was recorded on four occasions between 9 h 35 min 04 and 9 h 39 min 27 for about three seconds;
- noises similar to a person knocking on the cockpit door were recorded on six occasions between 9 h 35 min 32 (point) and 9 h 39 min 02;
- muffled voices were heard several times between 9 h 37 min 11 and 9 h 40 min 48, and at 9 h 37 min 13 a muffled voice asked for the door to be opened;
- between 9 h 35 min 07 and 9 h 37 min 54, the Marseille control centre tried to contact the flight crew on three occasions on 121.500 MHz, and on two occasions on 127.180 MHz, without any answer;
- between 9 h 38 min 38 and 9 h 39 min 23, an air traffic controller from the French Air Defence system tried to contact the flight crew on three occasions on 121.500 MHz, without any answer;
- noises similar to violent blows on the cockpit door were recorded on five occasions between 9 h 39 min 30 and 9 h 40 min 28;
- low amplitude inputs on the co-pilot’s sidestick were recorded between 9 h 39 min 33 and 9 h 40 min 07;
- the flight crew of another aeroplane tried to contact the flight crew of GWI18G at 9 h 39 min 54, without any answer.
- At 9 h 40 min 41, the ‘‘Terrain, Terrain, Pull Up, Pull Up’’ aural warning from the GPWS triggered and remained active until the end of the flight.
- At 9 h 40 min 56, a Master Caution was recorded, then at 9 h 41 min 00 the Master Warning triggered and remained active until the end of the flight.
- At 9 h 41 min 06, the CVR recording stopped at the moment of the collision with the terrain.
Source: Final Report, ¶1.1
3
Analysis
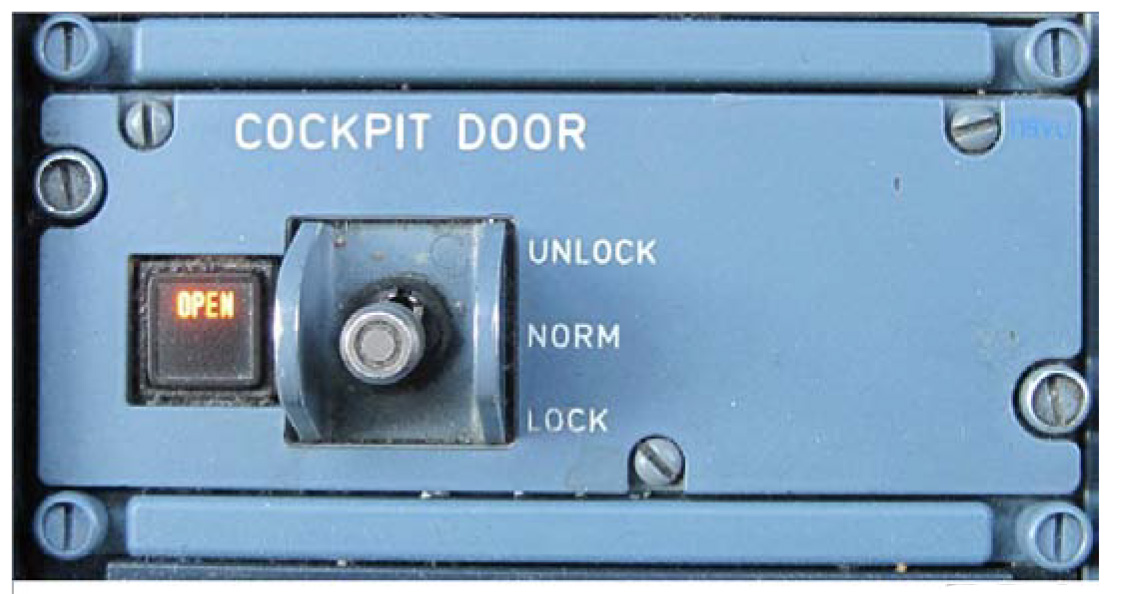
Cockpit door toggle switch, Final Report, figure 5.
We know what happened: the copilot planned a suicide using the captain's absence from the flight deck and a lockable cockpit door to turn his airplane into a projectile. They mystery is how the copilot, with years of mental health issues, was able to maintain a clearance for flight duties.
- A door separates the cockpit and passenger cabin. Its core consists of a composite sandwich type structure made of prepreg sheets covering a honeycomb core. The outer prepreg sheets are designed to ensure bullet-proofing. A door escape hatch is pre-cut on its lower part. The latter can only be used from the cockpit. It is used in emergencies when the door is stuck. Unlike the cockpit door which opens towards the inside of the cockpit, the door escape hatch can only be opened in the opposite direction.
- In case of emergency (suspected flight crew incapacitation, for example), the emergency access code can be dialled on the digital keypad. The acoustic signal then sounds continuously in the cockpit for 15 seconds and the green LED on the keypad starts to flash.
- If the flight crew does not respond within these 15 seconds, the door unlocks for 5 seconds. The green LED lights up continuously to indicate the door has been unlocked and the acoustic signal stops. The door only needs to be pushed in order to open it. After these five seconds have elapsed, the door locks again.
- If the flight crew toggles the switch during those 15 seconds, the acoustic signal stops and the system reacts according to the command (UNLOCK/LOCK).
Source: Final Report, ¶1.6.4
Source:
[Final Report, ¶1.13.1] Medical history of the copilot
- In August 2008, the co-pilot started to suffer from a severe depressive episode without psychotic symptoms. During this depression, he had suicidal ideation, made several “no suicide pacts” with his treating psychiatrist and was hospitalized.
- 09/04/2008 — Lufthansa AeMC — Issuance of the first class 1 medical certificate (no restrictions).
- He undertook anti-depressive medication between January and July 2009 and psychotherapeutic treatment from January 2009 until October 2009. His treating psychiatrist stated that the co-pilot had fully recovered in July 2009.
- 10/07/2009 — Treating psychiatrist — Report stating that the co-pilot is “entirely healthy” and that “the treatment has ended”.
- 14/07/2009 — Lufthansa AeMC — Application for the renewal of the class 1 medical certificate. This renewal was refused by the Lufthansa AeMC and the LBA was informed of this AeMC.
- 28/07/2009 — Luftansa AeMC — Issuance of the class 1 medical certificate with a waiver FRA 091/09, stating that it would become invalid if there were a relapse into depression.
- 11/08/2009 — Treating psychotherapist — Letter from the treating psychotherapist to confirm that the pilot could resume his flight training. This letter mentioned a severe depression, but initially had the reference code for recurrent depressive disorder. After this anomaly was detected by the AeMC, the psychotherapist re-issued the same letter with the correct code.
- 24/02/2105 — Treating psychiatrist — First prescription of Mirtazapine.
- 09/03/2015 — Private physician — Issurance of a sick leave certificate. This certificate was not forwarded to Germanwings.
From this point the class 1 medical was reissued repeatedly with the waiver.
From this point he was referred for psychiatric hospital treatment "due to a possible psychosis", issued two more sick leave certificates, and further prescribed Escitalopram, Dominal, and Zolipidem.
Depressive disorder
- The World Health Organisation defines depression as a common mental disorder, characterized by sadness, loss of interest or pleasure, feelings of guilt or low self‑worth, disturbed sleep or appetite, feelings of tiredness and poor concentration. It can be long lasting or recurrent, substantially impairing a person’s ability to function at work or school, or cope with daily life. At its most severe, depression can lead to suicide. When mild, depression can be treated without medicines but, when moderate or severe, people may need medication and professional talking treatments.
- Depression is one of the most common psychiatric disorders. According to several studies, about 10% of the general population has reported having experienced a period of depression in their life. Depressive disorders can occur at any age, including in childhood, but it appears for the first time more often in late adolescence or early adulthood.
- Depressive disorders and medications used to treat depression are usually medically disqualifying for pilots. Aviation authorities have not unified their approach on the consequences that the use of specific antidepressants and/or use of psychotherapy may have on pilot’s medical certification. Some regulatory authorities allow air crew on specific antidepressants, like a selective serotonin reuptake inhibitor (SSRI), to fly, although close medical follow-up is mandatory.
Psychotic disorder
- A psychotic disorder, or psychosis, is characterized by a loss of connectedness with reality, in the form of delusions, hallucinations, or disorganised thoughts. It may be chronic, intermittent, or occur in a single episode. It may also occur as accompanying symptoms in other psychiatric conditions including but not limited to bipolar disorder (e.g. bipolar disorder with psychotic features), major depression (e.g. major depression with psychotic features), or borderline personality disorder.
- Episodes of psychosis may be relatively brief due to an acute medical condition or the taking of a psychoactive substance (illicit or prescribed medication). Psychotic symptoms may also be chronic, possibly fading with time, but present to some degree in an ongoing manner, as seen in schizophrenia or schizoaffective disorder. Onset of chronic psychotic illness can occur at any age, with schizophrenia’s median onset age found to be in the mid-to-late 20s. Studies have shown that unless the patient shows evidence of a significant cognitive disorder in advance, the ability to identify these patients must wait until the onset of frank psychotic symptoms. The expert working group on mental health of the Aerospace Medical Association (AsMA) released recommendations in September 2012, and updated them in September 2015 after the Germanwings accident. They stated that serious mental illness such as acute psychosis was relatively rare, and its onset was difficult to predict.
- Acute psychotic disorders are generally addressed through a correction of the underlying cause. Brief courses of antipsychotic agents may be helpful if the patient represents a danger to self or others.
Cognitive constriction in suicides
- The American suicidologist Edwin Shneidman has described several common characteristics of suicide in his book “The Definition of Suicide” (1985). In particular, he wrote that the common cognitive state in suicide is constriction. Suicidal thoughts and plans are frequently associated with a rigid and narrow pattern of thinking that is comparable to tunnel vision and narrowing of focus. The suicidal person is temporarily unable or unwilling to engage in effective problem-solving behaviour and may see his or her options in extreme, all or nothing terms.
- According to Shneidman, people with high standards and expectations are especially vulnerable to ideas of suicide when progress toward these goals is suddenly frustrated. People who attribute failure or disappointment to their own shortcomings may come to view themselves as worthless, incompetent or unlovable.
Source: Final Report, ¶1.16.2] Mental issues
- Section 203 (1) of the German criminal code applies to health care personnel whose vocational training and professional title is state-approved (e.g. psychotherapists, physical therapists, care professions). It states that whosoever unlawfully discloses a secret of another, in particular, a secret which belongs to the sphere of personal privacy, which was confided to or otherwise made known to him in his capacity as a physician or member of another healthcare profession shall be liable to imprisonment not exceeding one year or a fine.
- If a holder of a medical certificate contacts his family doctor (GMP, etc.) or another physician, who detects an illness not compatible with the pilot duties or with flight safety, the contacted physician is not obliged to inform the responsible AME nor the employer nor the aviation authority. Due to medical confidentiality reasons, the information of third parties is impeded. The possibility to disclose aeromedical data depends upon the imminent danger resulting from the illness of the pilot concerned. Nevertheless the principle of confidentiality can prevent the treating doctor from disclosing such information.
- The inspection performed by EASA in July 2014 highlighted possible conflicts between German data protection laws and the application of Part-MED. It was found that the German data protection laws interfered with the oversight of AMEs and AeMCs, in particular:
- the personal medical data of aero-medical examinations performed by AMEs or AeMCs were not available to the LBA;
- the medical personnel from the LBA were prevented from examining and taking copies of the medical records or data relevant to the execution of the oversight task.
- The LBA responded to these findings and the December 2014’s amendment of the LuftPersV now allows the transfer of medical data to the LBA but it has to be done in an anonymous way.
Source: Final Report, ¶1.17.4] Medical certification process for flight crews in Germany
- All applicants with any of the following conditions must be denied or deferred to the FAA’s Federal Air Surgeon: attention deficit/hyperactivity, bipolar disorder, personality disorder, psychosis, substance abuse, substance dependence, suicide attempt. In some instances, the following conditions may also warrant denial or deferral: adjustment disorder; bereavement; dysthymic; minor depression; use of psychotropic medications for smoking cessation.
- The FAA has determined that airmen requesting first, second, or third class medical certificates while being treated with one of four specific antidepressant medications (Selective Serotonin Reuptake Inhibitors - SSRI) may be considered. The decision is made on a case-by-case basis. AMEs may not issue in those cases, it has to be done by the FAA.
Source: Final Report, ¶1.17.7] Medical certification process for flight crews in the USA
4
Cause
Those of us who have flown professionally for a while know that the cross section of the pilot population is much like that of the rest of the flying public, perhaps a bit more physically fit and mentally sound. But while our numbers of unfit are lower, they are not zero. One of the unintended consequences of the aftermath of the 9/11 terrorist attacks was the impenetrable cockpit door. One of the recommendations resulting from this crash was the insistence of having two people in the cockpit at all times. I'm not sure this will do any good because a person planning suicide will come up with measures to overcome this. What we are left with is a need for all crewmembers to keep an eye on other crewmembers.
- The collision with the ground was due to the deliberate and planned action of the co-pilot who decided to commit suicide while alone in the cockpit. The process for medical certification of pilots, in particular self-reporting in case of decrease in medical fitness between two periodic medical evaluations, did not succeed in preventing the co-pilot, who was experiencing mental disorder with psychotic symptoms, from exercising the privilege of his license.
- The following factors may have contributed to the failure of this principle: the co-pilot’s probable fear of losing his ability to fly as a professional pilot if he had reported his decrease in medical fitness to an AME; the potential financial consequences generated by the lack of specific insurance covering the risks of loss of income in case of unfitness to fly; the lack of clear guidelines in German regulations on when a threat to public safety outweighs the requirements of medical confidentiality.
- Security requirements led to cockpit doors designed to resist forcible intrusion by unauthorized persons. This made it impossible to enter the flight compartment before the aircraft impacted the terrain in the French Alps.
Source: Final Report, ¶3.2
References
(Source material)
Final Report, Accident on 24 March 2015 at Prads-Haute-Bléone (Alpes-de-Haute-Provence, France) to the Airbus A320-211 registered D-AIPX operated by Germanwings, Bureau d'Enquêtes et D'Analyses pur la sécurité de l'aviation civile