As with many of these accidents, the list of problems is pretty long, to include: hiring practices, a captain not adequately monitoring a first officer, and a first officer who apparently panicked to the point of shoving the nose down against the captain's efforts until outside visual reference finally convinced him the airplane wasn't in a stall; just to name a few.
— James Albright
Updated:
2024-08-15

Accident airplane,
Chairman's Factual Report, photo 1
I'll go through the accident report and cover much of what the NTSB thought noteworthy. But I would also like to cover a few extra points that bear extra consideration for those of us who fly airplanes professionally. First: startle factor. There is no doubt the first officer had a tendency to act first, ask questions second. Second: somatogravic illusion, the way our senses can be fooled by acceleration. Third: capability illusion, the normal pilot tendency to believe we are more capable than we are.
1
Accident report
- Date: 23 February 2019
- Time: 12:39
- Type: Boeing 767-375ER
- Operator: Atlas Air
- Registration: N1217A
- Fatalities: 2 of 2 crew, 1 of 1 passengers
- Aircraft Fate: Destroyed
- Phase: En route
- Airport: (Departure) Miami International Airport, FL (KMIA)
- Airport: (Destination) Houston-George Bush Intercontinental Airport, TX (KIAH)
2
Narrative
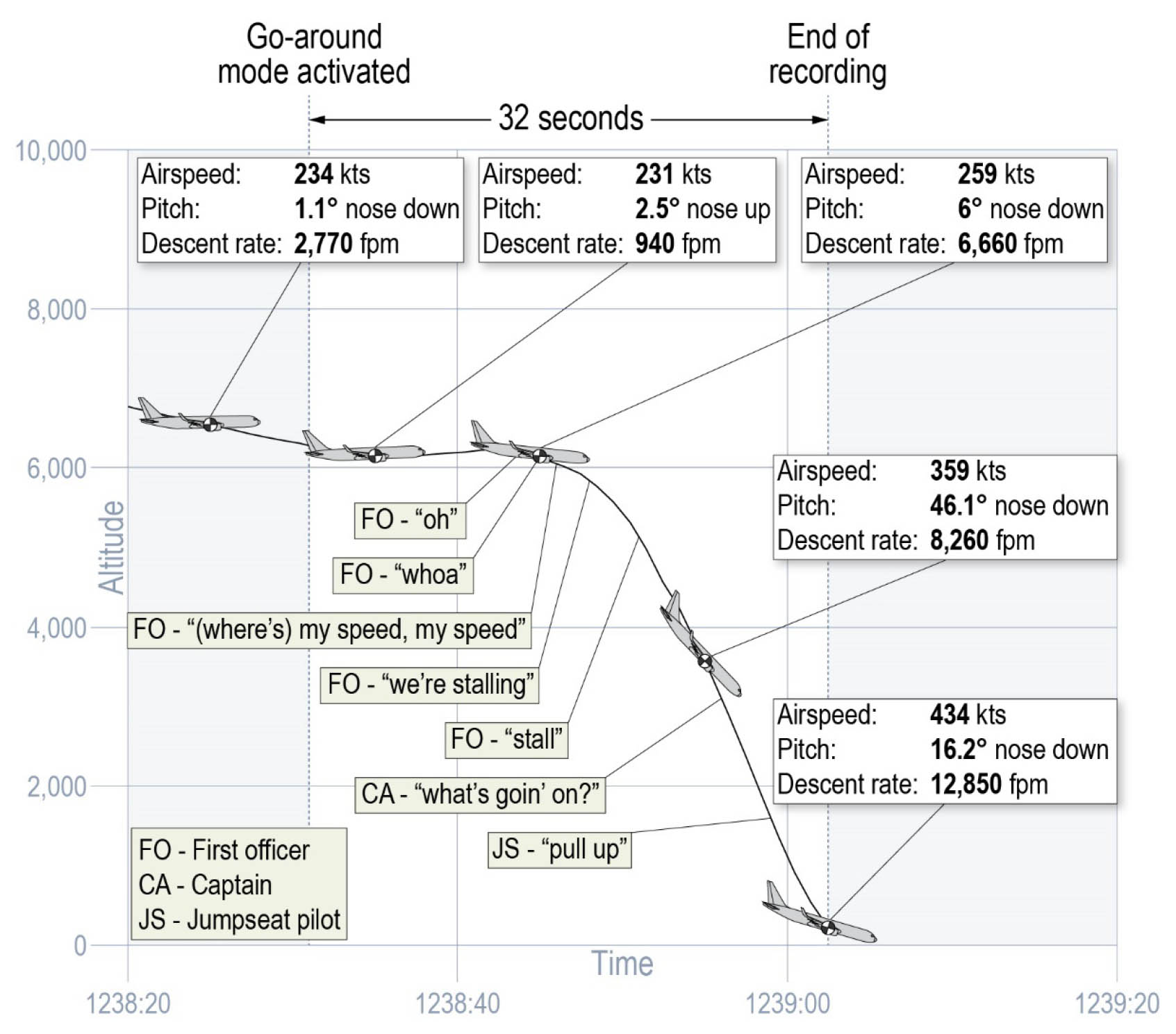
Final seconds of flight, NTSB AAR 2002, figure 1.
- On February 23, 2019, at 1239 central standard time, Atlas Air Inc. (Atlas) flight 3591, a Boeing 767-375BCF, N1217A, was destroyed after it rapidly descended from an altitude of about 6,000 ft mean sea level (msl) and crashed into a shallow, muddy marsh area of Trinity Bay, Texas, about 41 miles east-southeast of George Bush Intercontinental/Houston Airport (IAH), Houston, Texas. The captain, first officer (FO), and a nonrevenue pilot riding in the jumpseat died. Atlas operated the airplane as a Title 14 Code of Federal Regulations (CFR) Part 121 domestic cargo flight for Amazon.com Services LLC, and an instrument flight rules flight plan was filed. The flight departed from Miami International Airport (MIA), Miami, Florida, about 1033 (1133 eastern standard time) and was destined for IAH.
- A review of cockpit voice recorder (CVR) and flight data recorder (FDR) data determined that the flight’s departure from MIA, en route cruise, and initial descent toward IAH were uneventful. The FO was the pilot flying (PF), the captain was the pilot monitoring (PM), and automated flight functions (autopilot and autothrottle) were engaged. At 1230:37, when the flight was about 73 miles southeast of IAH and descending normally through about 17,800 ft msl, the captain checked in with the Houston terminal radar approach controller and reported that the flight was descending toward the airport on the assigned arrival route. At 1234:09, the approach controller advised the flight crew of an area of light-to-heavy precipitation about 35 miles ahead of the flight’s position and that they could expect vectors to navigate around it.
- The FDR data showed the flight continued to descend normally on the assigned arrival route. According to CVR audio, at 1236:07, the FO said, “okay – I just had a…,” then, 3 seconds later, he initiated a positive transfer of airplane control to transfer PF duties to the captain, stating, “your controls.” The captain responded, “my controls.” At 1237:07, the FO made a comment about the electronic flight instrument (EFI) switch. Two seconds later, the FO said, “okay, I got it back,” and the captain said, “now it’s back.” The FO then said, “I press the EFI button, it fixes everything,” and the captain acknowledged.
- While acting as PM, the FO advised the air traffic controller that the flight would like a vector west of the weather and acknowledged the controller’s instructions for the flight to “hustle all the way down” in its descent to 3,000 ft msl. As the airplane continued its descent, the speedbrakes were extended. The controller advised the flight to turn left to 270°, which the captain acknowledged before transferring PF duties back to the FO at 1237:24.
Source: NTSB AAR-20/03, §1.1
The crew had been debating which way to turn to avoid the weather system directly in front. A turn to the west would be toward the airport. A turn to the east would add considerable distance. While the FO was acting as PM, the controller at first said west would be a problem because of departures. The crew agreed to go east, since fuel was not a factor. Then the controller said he could get them to the west, provided they "hustle all the way down."
The CA was flying the aircraft when the "hustle all the way down" instruction was given. It is likely that the CA pulled the speedbrake lever. Atlas SOP calls for the PF to keep his or her hand on the speedbrake lever when it is deployed, but we don't know if this was done.
- After the FO resumed PF duties, the CVR recorded comments between the FO and the captain that were consistent with setting up the flight management computer (FMC) and configuring the airplane for the approach to IAH, including lowering the slats (consistent with the “flaps 1” setting). The FDR data showed that the airplane continued to descend normally until 1238:31, when the airplane’s go-around mode was activated. At the time, the airplane was about 40 miles from IAH at an altitude about 6,300 ft msl.
Source: NTSB AAR-20/03, §1.1
It appears the CA was heads down programming the FMC while the FO was flying. The CA was attempting to get a course to the airport to allow the FMC to show a VNAV path, but they were on an assigned heading so that could not have worked. The CA figured it out but there was some confusion for a few seconds.
- 12:38:02.2 HOT-2 'kay flaps one.
- 12:38:04.8 CAM [Sound of mechanical click.]
- 12:38:05.1 HOT-2 thank you.
- 12:38:06.1 HOT-1 confirm. confirm.
- 12:38:07.3 HOT-2 execute.
- 12:38:08.7 HOT-1 LNAVs available.
- 12:38:09.9 HOT-2 LNAV is...
- 12:38:14.3 HOT-1 not on intercept heading.
- 12:38:15.0 HOT-2 no (your on/it's on) a heading right?
- 12:38:31.1 CAM [Sound of click.]
Source: NTSB AAR-20/03, Cockpit Voice Recorder
The NTSB Sound Spectrum Study concluded that the sound of the click may have been the GA button being pressed, though the sound was degraded to the point that the evidence was not conclusive. While this happened, the CA heard and responded to a radio call.
- 12:38:35.1 APP Giant thirty-five ninety-one in about another eighteen miles or so we'll cut you due north(bound) for a base leg.
Source: NTSB AAR-20/03, Cockpit Voice Recorder
- During the next 6 seconds, the airplane’s automated flight functions commanded nose-up pitch and an increase in engine thrust, consistent with go-around mode-driven commands. Neither crewmember made any callout to indicate intentional activation of the go-around mode or took action to disconnect the automation. The captain continued to receive and respond to routine air traffic control (ATC) communications.
- About 1238:36, the speedbrakes were retracted, then the airplane’s elevators moved in response to manual control inputs to command nose-down pitch. The amount of nose-down pitch continued to increase, and the airplane entered a steep descent.
Source: NTSB AAR-20/03, §1.1
It appears the CA's attention was on the radio while all this was happening. The speedbrake movement happened five seconds after the TO/GA activation and in concert with the nose pitch down.
- 12:38:40.3 CAM [Sound of four beeps within a duration of .75 seconds at a frequency of 1200 Hz.]
- 12:38:41.4 RDO-1 sounds good uh Giant thirty-five ninety-one.
- 12:38:43.6 APP it is severe clear on the other side of this stuff so you'll have no problem gettin' the airport *(either).
Source: NTSB AAR-20/03, Cockpit Voice Recorder
The NTSB Sound Spectrum Study did not conclusively identify the sound of the four beeps but mentioned that it was consistent with an "owl" beeper used for all system alert caution messages.
- Beginning at 1238:44, the FO said, “oh,” then said in an elevated voice “whoa… (where’s) my speed, my speed…we’re stalling;” he then exclaimed “stall” at 1238:51. A review of FDR data determined that the airplane’s airspeed and pitch parameters were not consistent with the airplane at (or near) a stalled condition, and none of the stall warning system indications activated.
Source: NTSB AAR-20/03, §1.1
- 12:38:47.3 RDO-1 okay.
Source: NTSB AAR-20/03, Cockpit Voice Recorder
- At 1238:56, the captain asked, “what’s goin’ on?” Three seconds later, the pilot riding in the jumpseat shouted, “pull up.” About this time, the elevators moved consistent with manual control inputs to command airplane nose-up pitch. The nose-up pitch control inputs were held for the remaining 7 seconds of the flight but were unsuccessful in arresting the airplane’s descent in time to prevent its crash into the marsh (see figure 1).
Source: NTSB AAR-20/03, §1.1
The time between the CA ending his radio conversation and his "what's goin' on" statement was about 8 seconds, which might indicate the time it took for him to assess the situation.
3
Analysis
The Captain
The captain, age 60, held an airline transport pilot (ATP) certificate with type ratings for Boeing 757, Boeing 767, and Embraer ERJ145 airplanes. The captain was hired by Atlas as an FO on September 7, 2015, and he upgraded to captain on the Boeing 767 on August 25, 2018. At the time of the accident, the captain had accumulated about 11,172 hours of total flying time, of which 4,235 hours were as pilot-in-command (PIC). He had a total of 1,252 hours of flying time in Boeing 767-series airplanes, of which 157 hours were as PIC.
On October 31, 2015, the captain (while an FO) was not recommended for his Boeing 767 type-rating checkride after he allowed the airplane’s airspeed to exceed the specified limitation for the flaps during stall recovery, consistently failed to set the missed approach altitude, and had problems performing missed approach procedures. He satisfactorily completed remedial training the next day, which included speed awareness during recovery from approaches to a stall. On November 2, 2015, he completed his Boeing 767 type-rating checkride, which included an evaluation of a takeoff stall during a turn.
As a result of the October 2015 training failures associated with the captain (as an FO) not being recommended for the type-rating checkride, Atlas placed the captain in the pilot proficiency watch program (PWP) from November 11, 2015, until February 22, 2017. He completed recurrent training for the Boeing 767 on February 25, 2016, which included three stalls (takeoff, landing, and clean configurations), and proficiency checks on May 19, 2016, and September 5, 2016, each of which included one takeoff stall in a turn.
On August 12, 2018, the captain (while an FO) completed Boeing 767 captain-upgrade ground training, which included a 2-hour module on crew resource management (CRM, as required by 14 CFR 121.427) and an 8-hour module on captain leadership. He completed upgrade systems training on August 15, 2018, and was recommended for captain upgrade on August 23, 2018, after completing five upgrade training sessions in the full-flight simulator. He passed a captain proficiency check on August 25, 2018.
Source: NTSB AAR-20/03, §1.2
Note that the captain didn't have any heavy aircraft experience until being hired by Atlas four years earlier in his middle fifties. He had over 10,000 total hours flying aircraft no larger than the ERJ145. His early Atlas training failures reflect a pilot who wasn't able to grasp the finer points of dealing with heavy aircraft. At the time of the accident, he only had six months experience and 157 hours as a captain in the Boeing.
I think the captain's lack of experience in heavy aircraft was a factor in the accident, as I'll discuss below under Somatogravic Illusion.
The First Officer
- ATP Boeing 767, practical test failure (September 22, 2017): Takeoff and departure phase, in-flight maneuvers. Certificate issued 4 days later.
- ATP Embraer ERJ145, practical test failure (May 11, 2014): Nonprecision approaches, navigation procedures. Certificate issued the next day with a PIC limitation. The limitation was removed on September 30, 2014.
- ATP Embraer ERJ145, oral examination failure (April 22, 2014): Retest completed 4 days later.
- Mesa Airlines (February 2015 until July 2017, when he was hired by Atlas): Embraer ERJ175 FO, unsuccessfully attempted to upgrade to captain in May 2017 and resigned (citing “career growth”) to accept a position with Atlas.
- Trans States Airlines (March to September 2014): Embraer ERJ145 FO, failed an oral examination for the Embraer ERJ145 in April (then successfully retested) and failed Embraer ERJ145 ATP checkride in May (then successfully received his certificate). He was graded unsatisfactory on a line check in August and resigned citing personal reasons.
- Charter Air Transport (February 2013 to March 2014): Embraer EMB120 FO.
- Air Wisconsin Airlines (April to August 2012): Did not complete FO initial training for Canadair Regional Jet and resigned citing personal reasons.
- CommutAir (May to June 2011): Did not complete FO initial training for de Havilland DHC-8 and resigned citing “lack of progress in training.”
- Air Turks and Caicos (June 2008 to June 2010): Embraer EMB120 FO until furloughed.
- §E, ¶3.2. Atlas Air Interview Process
The FO, age 44, held an ATP certificate with type ratings for Boeing 757 and 767 airplanes and Embraer EMB120, ERJ145, ERJ170, and ERJ190 airplanes. The FO was hired by Atlas on July 3, 2017, and transitioned to and received his initial type rating on the Boeing 767 on September 26, 2017. At the time of the accident, the FO had accumulated about 5,073 hours total flying time, of which 1,237 hours were as PIC. He had accumulated a total of 520 hours of flying time as second-in-command in Boeing 767-series airplanes.
The FO completed Atlas basic indoctrination training on July 7, 2017, and Boeing 767 ground school on July 22, 2017. On July 27, 2017, he was not recommended for his Boeing 767 type-rating oral examination due to his need for remedial training in takeoff and landing performance and airplane systems. He completed 4.5 hours of remedial training, which included takeoff and landing performance and aircraft systems, then passed the oral examination on July 29, 2017. The FO was recommended to begin Boeing 767 fixed-base simulator training the next day. After completing five fixed-base simulator training sessions, the FO was not recommended to proceed to full-flight simulator training due to his difficulty in completing normal procedures. The FO received one 4-hour remedial training session then completed fixed-base training on August 8, 2017.
On September 22, 2017, the FO failed his practical Boeing 767 type-rating examination due to unsatisfactory performance in CRM, threat and error management, nonprecision approaches, steep turns, and judgment. During a postaccident interview, the Atlas check airman who was the FO’s examiner said the FO was very nervous, had “very low” situational awareness, overcontrolled the airplane, did not work well with the other pilot, omitted an emergency checklist during an abnormal event, and exceeded a flap speed. The examiner said the FO was not thinking ahead, and, when he realized that he needed to do something, he often did something inappropriate, like push the wrong button. The examiner said the FO’s performance was so poor that he worried that the FO would be unable to “mentally recover” enough to complete the course.
The FO received remedial training on September 25, 2017, and he passed the type-rating checkride the next day. During a postaccident interview, the Atlas instructor who performed the FO’s remedial training (who was not the same person as the checkride examiner) said he thought the FO had a confidence problem and described the remedial training as a “great training session.” The FO was not placed in the PWP.
FAA records for the FO showed no reports of any previous aviation accidents or incidents. Records for the FO’s pilot certificates showed the following notices of disapproval (and subsequent certificate issuances after he passed retests):
The FO’s previous employment included the following:
When the FO applied for a job at Atlas, he did not disclose that he had worked for Air Wisconsin and CommutAir or that he did not complete initial training at either airline. He also did not disclose to Trans States Airlines when he applied for a job there that he had previously worked for and did not complete initial training at Air Wisconsin. Investigative interviews with instructors who evaluated the FO at two of his previous employers provided insight into the FO’s training performance at those airlines.
According to one check airman at Mesa Airlines, the FO could explain things well in the briefing room and performed some expected tasks well in the simulator. However, when presented with something unexpected in the simulator, the FO would get extremely flustered and could not respond appropriately to the situation. She said that when the FO did not know what to do, he became extremely anxious and would start pushing a lot of buttons without thinking about what he was pushing, just to be doing something. She noted that the FO lacked an understanding of how unsafe his actions were, and he could not see why he should not be upgraded to a captain.
Another check airman at Mesa said the FO’s stick and rudder skills were weak, and he also struggled with basic flight management system tasks. This check airman described the FO’s piloting performance as among the worst he had ever seen and noted that the FO tended to have an excuse for each of his poor performances, such as blaming his simulator partner, his instructor, or the hotel. A third check airman at Mesa said that the FO had weak situational awareness, did not realize what was going on with the airplane at times, and had difficulty staying ahead of the airplane. She said the FO was completely unaware that he lacked skills, unwilling to accept feedback, and unhappy with her about his failure to upgrade to captain.
An instructor who taught cockpit procedures on the flight training devices at Air Wisconsin Airlines recalled that during one emergency procedures training scenario, the FO made abrupt control inputs that triggered the stick shaker and overspeed alerts. The instructor said that instead of staying engaged in the scenario and addressing the problem with his training partner, the FO just stopped what he was doing and turned around and looked at the instructor. The instructor found this reaction highly unusual.
According to the Director of HR, in the last year Atlas Air received 1,200 to 1,400 pilot applications, which had declined in the past years from a previous 3,000 applications per year. Since about 2015, Atlas Air had been hiring about 300 pilots each year, and for 2019 Atlas and Southern Air were scheduled to hire about 700 pilots (split about evenly). She stated that in the last 3 years, they had seen a “tough pilot market” with the current pilot shortage.
Source: NTSB AAR-20/03, §1.2
The first officer's record shows he managed to fail up from one airline to another until he got to Atlas, where he appeared to show some staying power. He had been with the company for a year and a half. The records show he had over 1,200 hours as a PIC, but it appears he never made captain while flying commercially. His records do show multiple attempts and failures to upgrade.
I think the first officer's track record of failure, blaming others for that failure, and subsequent success at getting new airline jobs may have fed the illusion that he actually knew what he was doing. He was one of those pilots who not only "didn't know," he also "didn't know what he didn't know." As I will discuss below, he had a capability illusion.
- Atlas’ procedures for considering pilot applicants included an initial review for minimum requirements, resume review, and initial telephone screening with a recruiter before an interview would be scheduled. Atlas’ HR director and the senior director of flight procedures, training, and standards (director of training) said the application process relied on the applicants’ honesty in disclosing information. The HR director said the process included crosschecking to ensure that information provided during interviews, on the application, and in the background check all agreed but noted that “it’s hard to catch someone who’s deliberately trying to deceive you.”
- When the accident FO applied for a job at Atlas, he did not disclose that he had worked briefly for and resigned from both CommutAir (in 2011) and Air Wisconsin Airlines (in 2012). The FO stated on his Atlas employment application that gaps in his employment history were times when he was furloughed, working as a freelance real estate agent, or attending college. Atlas’ director of training said he would have liked to have known about the FO’s work history at CommutAir and Air Wisconsin Airlines during hiring so he could have further evaluated trends in the FO’s training. He considered an applicant’s failure to disclose employer information as deceptive and possibly grounds for termination if discovered after hire.
Source: NTSB AAR-20/03, §1.
The Pilot Records Improvement Act (PRIA) was enacted in 1996 to prevent these kinds of things from happening. PRIA, more or less, depended on pilots faithfully presenting their records. After the Colgan Air 3407 accident in 2009, the NTSB recommended the FAA institute a Pilots Records Database that would give employers an easy way to check pilot records. Congress finally mandated this to take place on April 30, 2017, but it never got done. Forty days later his Atlas hired this first officer. As I write this, the PRD is still not in placed but is promised for September 2024.
The "Go around"
Go-Around Switches. The airplane’s go-around switches were located on the outboard underside of each thrust lever. Internally, each go-around switch contained a set of three microswitch contacts that provided discrete inputs to various computers for the automated flight system. To activate the go-around mode, a pilot would typically use the thumb of the hand that is holding the thrust levers to push the nearest switch.18 The speedbrake lever was located to the left of the thrust levers (see figure 7).
Source: NTSB AAR-20/03, §1.3.2
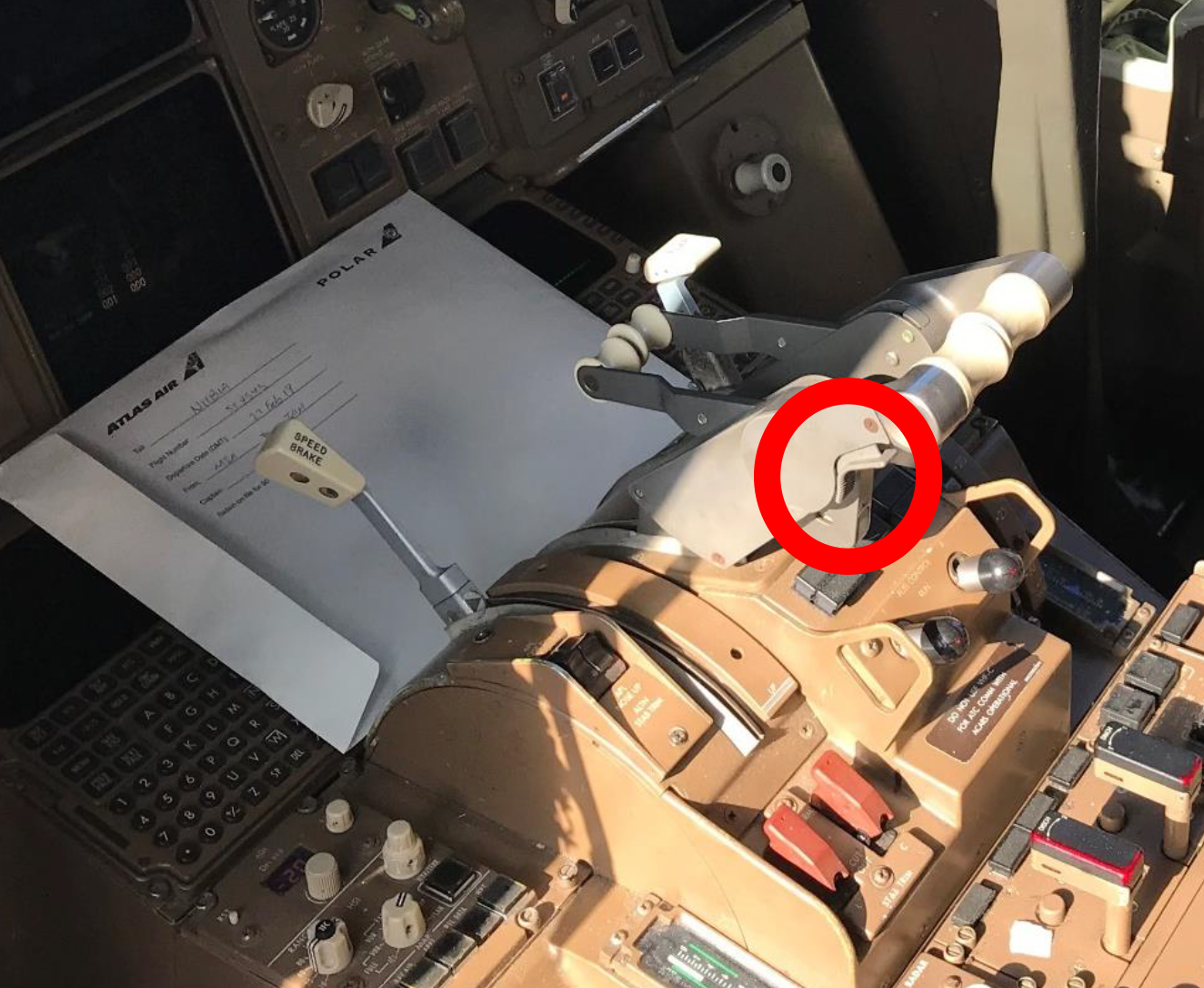
Go around switches, NTSB AAR 20/02, figure 7.
- Before the go-around mode was activated, the airplane was descending normally at a reduced thrust setting (thrust levers were about 32° to 33°) with an airplane pitch attitude of about 1° nose down and operated with the autopilot and autothrottle engaged. The airplane’s automated flight control system could perform climb, cruise, descent, and approach functions as selected by the flight crew using the mode control panel (MCP), FMC, and thrust mode selector. The FDR data indicated that the crew had the assigned altitude of 3,000 ft msl selected using the MCP.
- FDR data showed that airplane vertical load factor variations began about 1238:25, with a peak vertical acceleration of 1.26 gravitational acceleration (g); as described in section 1.4, the flight was in the immediate vicinity of the leading edge of a cold front at the time. FDR data at 1238:31 showed that the airplane’s automated flight system status for the go-around mode changed to “activated,” and the CVR recorded a “click” at this time.
- In the accident airplane’s configuration with autopilot and autothrottle engaged, the autopilot/flight director system (AFDS) and autothrottle would be expected to respond by controlling airplane pitch, roll, and thrust to maintain ground track, hold the existing airspeed, and establish a climb rate of at least 2,000 ft per minute. During the next 6 seconds, automated flight commands advanced the thrust levers to about 80° to 82°, resulting in increased thrust and longitudinal acceleration, and moved the control column and elevators to command nose-up pitch; during this time, the airplane’s pitch increased to about 4° nose up.
- About 1238:36, the speedbrake lever was moved from the extended position to the armed position, which retracted the speedbrakes. Recorded airplane parameters at this time, including those for air/ground sensing and flap setting criteria, did not meet the conditions for automatic speedbrake retraction.
- Between about 1238:38 to 1238:56, the airplane pitched nose down and continued to accelerate, reaching a peak longitudinal acceleration of 0.27 g at 1238:42. During this time, the position of the left elevator control column (the only side for which the FDR recorded position data) matched the position of the elevators, which was consistent with the elevators responding to manual inputs from a crewmember on an elevator control column. Such a manual override of the autopilot would require control column inputs in excess of 25 lbs. The airplane’s nose-down pitch during this time progressed rapidly to about 49° nose down, and the airplane entered a steep descent. At 1238:40, the CVR recorded a beeping sound consistent with the “owl” beeper; the FO then said, “oh” at 1238:44 and “whoa” at 1238:45.
- Between 1238:46 and 1238:56, the right elevator was in a more airplane nose-down position than the left elevator, which would be consistent with the captain and the FO each applying differing manual inputs on their respective control columns. At 1238:48 and 1238:51, the FO stated that the airplane was stalling. Review of the airplane’s recorded vane angle of attack (AOA), which was below -15°, and airspeed, which was above 250 knots (kts), determined that the airplane’s wing stall AOA was not exceeded, and the airplane was not at or near a wing-stalled condition. Also, the FDR’s recorded parameter for the stick shaker did not record the stick shaker as being active at any point in the flight.
- Beginning about 1238:45, the thrust levers were reduced to 33° within 1 second then increased to about 80° to 85° within 2 seconds. These rates of thrust lever movement were faster than the autothrottle system could command. At 1238:56, the captain asked, “what’s goin’ on?” At the time, the airplane was descending through an altitude of about 3,000 ft msl, and both elevators began to move concurrently toward an airplane nose-up position. About 2 seconds later, both elevators attained the full airplane nose-up position and remained there until the end of the FDR recording. During this time (beginning at 1238:56), a series of beeps consistent with the “siren” sounded, and the FDR recorded an overspeed.
- Just before the FDR recording ended at 1239:03, the airplane’s pitch was about 20° nose down, its airspeed was in excess of 400 kts, and its load factor was more than 4 g.
Source: NTSB AAR-20/03, §1.8
If you are well versed at practicing a go around using a typical TO/GA system while at minimums in a smaller jet, you might be wondering why the captain didn't immediately react to the sudden acceleration from all that thrust and the huge pitch change from negative a few degrees to positive a lot of degrees. This TO/GA occurred at over 6,000 feet where available thrust is somewhat reduced. Even more significant than that is the factor of the size and mass of the airplane. The feel of acceleration in a 767 in this situation will be quite a bit subdued compared to a smaller jet. At the time TO/GA was hit, the aircraft had a pitch of 1.1 degrees nose down. The maximum pitch after TO/GA was 2.5 degrees nose up, and increase of only 3.6 degrees. They were in moderate turbulence, which would further mask any noise, vibration, and pitch change. The time from TO/GA activation to the end of the CVR was only 32 seconds. The captain, at that moment, had been trying to diagnose why the FMC didn't react to his programming changes, listening to a radio call, and responding to that call. The time from the TO/GA activation to the captain's "What going on?" question was 25 seconds. There can be no doubt that everyone in the cockpit were victims of startle factor.
The NTSB seems to think the FO accidentally activated the TO/GA button with his forearm while reaching for the speedbrake handle. I'm not so sure, as the TO/GA appeared to be activated five seconds before the speedbrake handle made it to the closed/armed position. It could be that in an effort to be smooth, the FO slowly pushed the speedbrake handle forward. But I've flown aircraft where the timing of the boards was mandated in some situations to be no faster than 3 seconds. That is a long time. I think it more likely that the FO activated the TO/GA in response to the failure to engage LNAV. As nonsensical as that might sound, he had a history of pushing random buttons when confronting unexpected situations.
- Within seconds of go-around mode activation, manual elevator control inputs overrode the autopilot and eventually forced the airplane into a steep dive from which the crew did not recover. Only 32 seconds elapsed between the go-around mode activation and the airplane’s ground impact.
- Atlas’ pilot training and procedures prescribed that, during operations with automated flight control systems engaged and the speedbrakes extended, the PF should keep one hand on the speedbrake lever as a reminder to retract the speedbrakes upon the autopilot’s capture of the selected altitude and associated automatic increase in thrust. Thus, the FO (as PF) likely had his hand on the speedbrake lever in accordance with Atlas’ guidance and in anticipation of retracting the speedbrakes once the airplane began to level off at its target altitude of 3,000 ft msl.
- Simulator observations of pilots performing this scenario showed that, for a PF in the right seat, holding the speedbrake lever can place the left hand and wrist under the thrust levers and close to the left go-around switch such that very little upward arm movement would be needed to make contact with the switch. For the accident flight, the effects inside the airplane during its encounter with light turbulence at the time the go-around mode was activated could be sufficient to move a crewmember’s arm this small distance. Therefore, the NTSB concludes that, presuming that the FO was holding the speedbrake lever as expected in accordance with Atlas’ procedure, the inadvertent activation of the go-around mode likely resulted from unintended contact between the FO’s left wrist or watch and the left go-around switch due to turbulence-induced loads that moved his arm.
- The unexpected mode change associated with the inadvertent go-around mode activation (and the higher altitude at which it occurred) would have been recognizable to the FO and the captain through an effective instrument scan. Both the flight mode annunciator and the engine indicating and crew-alerting system (EICAS) would have displayed “GA” indications, and the altimeter would have indicated about 6,300 ft msl.
- Although the FO did not verbalize awareness that something unexpected had happened until about 13 seconds after go-around mode activation (when he said “oh” and then “whoa” in an elevated voice), manual control inputs that began sooner suggest that the FO (as PF) had sensed changes in the airplane’s state and had begun to react without fully assessing the situation.
- The manual retraction of the speedbrakes 5 seconds after go-around mode activation was likely performed by the FO (as PF) instinctively once he felt the increased load factor from the airplane leveling off and heard and felt the engine thrust increasing. He had likely been anticipating the need to perform this task when the airplane leveled off.
- However, beginning about 1 second later, as the airplane’s acceleration and upward pitch began to increase (which would have resulted in the aft movement of the GIF vector sensed by the pilots), manual forward control column inputs were applied, overriding the small, autopilot-driven pitch-up command and resulting in decreasing pitch. Thus, the NTSB concludes that, given that the FO was the PF and had not verbalized any problem to the captain or initiated a positive transfer of airplane control, the manual forward elevator control column inputs that were applied seconds after the inadvertent activation of the go-around mode were likely made by the FO. Further, the captain was communicating with an air traffic controller at the time, consistent with his PM duties.
Source: NTSB AAR-20/03, §2
GIF: Gravito-Inertial Force. It is basically your body's sense of gravity which can be the earth's gravity, the translational force your body feels from acceleration, or a combination of the two.
- The human body uses three integrated systems to determine orientation and movement in space: vestibular (otolith organs in the inner ear that sense position), somatosensory (nerves in the skin, muscles, and joints that sense position based on gravity, feeling, and sound), and visual (eyes, which sense position based on sight). The vestibular and somatosensory systems alone cannot distinguish between acceleration forces due to gravity and those resulting from maneuvering the airplane.
- Thus, when visual cues are limited and an airplane rapidly accelerates or decelerates, a pilot may be susceptible to a somatogravic illusion (FAA 2016, 17-6). Somatogravic illusion is a form of spatial disorientation that results from a false sensation of pitch due to the inability of the otolith organs of the human inner ear to separate the gravitational and sustained linear acceleration components of the GIF vector (Young 2003 and Cheung 2004). Rapid acceleration in an airplane stimulates the otolith organs in the same way as tilting the head backward and may lead a pilot to mistakenly believe that the airplane has transitioned to a nose-up attitude (FAA 2016, 17-7).
- The accident airplane was likely flying in IMC when the go-around mode was activated. The timing of the FO’s subsequent nose-down control inputs correlated with increases in the airplane’s longitudinal acceleration associated with the go-around mode-commanded increase in engine thrust and retraction of the speedbrakes. This relationship suggests that the FO experienced a pitch-up somatogravic illusion at that time.
- Somatogravic illusion has long been recognized as a significant hazard that is likely to occur under conditions of sustained linear acceleration when outside visual references are obscured (Buley and Spelina 1970, 553-6). Further, such conditions can degrade a pilot’s ability to effectively scan and interpret the information presented on primary flight displays. For a pilot flying in IMC with no external visual horizon, maintaining spatial orientation when presented with conflicting vestibular cues depends upon trusting the airplane’s instruments and disregarding the sensory perceptions (FAA 2003). However, for some pilots (particularly those who are not proficient with maintaining airplane control while referencing only instruments), the introduction of misleading vestibular cues can be compelling enough that the pilot may find it difficult to accurately assess or believe reliable sources of information about airplane attitude, such as the airplane’s instruments. Thus, the NTSB concludes that the FO likely experienced a pitch-up somatogravic illusion as the airplane accelerated due to the inadvertent activation of the go-around mode, which prompted him to push forward on the elevator control column.
- After the FO began pushing forward on the control column and the airplane’s pitch dropped below the horizon, its vertical acceleration rapidly decreased. Due to this change and the airplane’s continued longitudinal acceleration, the resultant GIF vector sensed by the pilots swung dramatically aft. This likely exacerbated the FO’s pitch-up sensation and possibly produced a sensation of tumbling backward, known as the inversion illusion (Cheung 2004). The FO’s comments “oh” and “whoa,” which expressed surprise, likely reflected his experience of one or both phenomena.
Source: NTSB AAR-20/03, §2
4
Cause
The NTSB determines that the probable cause of this accident was the inappropriate response by the first officer as the pilot flying to an inadvertent activation of the go-around mode, which led to his spatial disorientation and nose-down control inputs that placed the airplane in a steep descent from which the crew did not recover. Contributing to the accident was the captain’s failure to adequately monitor the airplane’s flightpath and assume positive control of the airplane to effectively intervene. Also contributing were systemic deficiencies in the aviation industry’s selection and performance measurement practices, which failed to address the first officer’s aptitude-related deficiencies and maladaptive stress response. Also contributing to the accident was the Federal Aviation Administration’s failure to implement the pilot records database in a sufficiently robust and timely manner.
Source: NTSB AAR-20/03, §3.2
5
A deeper dive into why this accident happened
Startle response

Startled pilot
Flight Safety Foundation
The NTSB Report does mention that startle response may have been a factor in the first officer's behavior and that is true enough. But what is startle response? There isn't much written on startle response in aviation accidents, other than to say it happens, it causes pilots to act irrationally and against training, and there isn't much you can do about it.
While definitions vary, they all pretty much boil down to this: Startle response (or reflex or factor, etc.) is an involuntary response to a sudden or threatening stimuli. It is a neurological and physiological reaction that bypasses the brain's conscious decision making process. Some will tell you it is rare in pilots, but I think it more likely that most pilots are never presented with the circumstances that would prompt the startle response.
There have been studies and other attempts to train pilots to deal with startle response. For example: Training for Startle, FlightSafety Foundation. I suppose any effort to train is better than no effort, but I am not sure these methods are sufficient. In some of these attempts, pilots are made aware of the problem in a classroom, given several simulator exercises where there will be a surprise at some point. Those with the classroom do marginally better than those without and the scientists pat themselves on their backs and say job done. I don't think so. These startle students are in an academic environment with no risk or threat of consequences.
Is there a solution? I believe there is and that solution has been used with great success for a very long time. More about this: Startle Reponse.
Somatogravic illusion
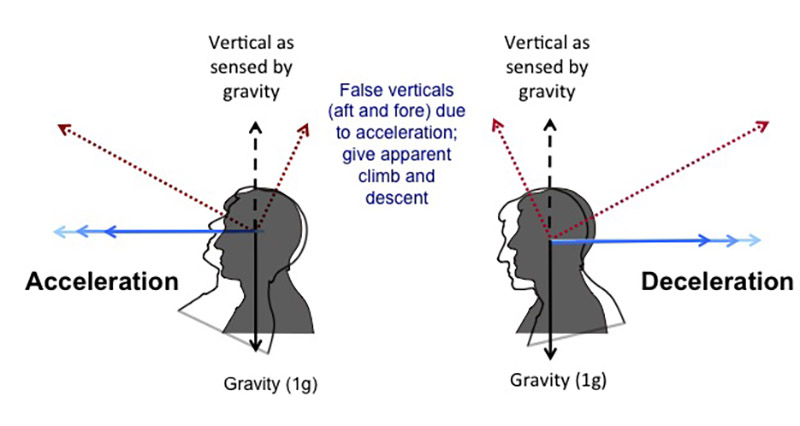
Somatogravic illusion, www.skybrary.aero.
The NTSB report hypothesizes that the First Officer may have hit the TO/GA switch located on the aft portion of the thrust levers, while he was moving the speedbrake handle which is left of those thrust levers. That is certainly possible. He was also known to activate random buttons and switches when under stress. Either way, you might be asking how he failed to notice the acceleration and pitch up of the aircraft that resulted from the TO/GA. Also, how did the Captain fail to notice that?
As I've mentioned above, the feel of acceleration in a 767 in this situation will be quite a bit subdued compared to a smaller jet. The pitch up was also subdued, only 3.6 degrees in total. Still, there was some acceleration and some pitch up. So why didn't these sensations trigger either pilot to immediately think the TO/GA had been activated? And beyond that question, why did the First Officer feel the aircraft was pitched up in a stall? Finally, why didn't the Captain sense the dramatic pitch down induced by the First Officer?
I think the combination of the turbulence, the steepening descent, and the activation of the speedbrakes played havoc with both pilots' sense of equilibrium in a way that should be familiar to most instrument rated pilots with experience in large aircraft flying in this kind of weather. Then the sensations compounded: the action of the pitch down, the deceleration caused by the speedbrakes follow by the acceleration caused by TO/GA thrust, the pitch up from TO/GA, and finally the pitch down caused by the First Officer. A few of the illusions that might be a factor in this accident:
- Oculugravic illusion. An acceleration or deceleration can cause the otolith organs in the inner ear to sense a nose high or nose low pitching motion, respectively.
- Somatogravic illusion. The somatosensory system is often called the "seat of the pants" feeling, since it takes from your skin, joints, and muscles. The effect of acceleration and deceleration is similar to that from the oculugravic illusion.
- Elevator illusion. An abrupt upward or downward vertical acceleration can create the illusion of being in a climb or descent.
- Inversion illusion. An abrupt change from a climb to straight and level flight can create the sensation of tumbling backwards.
More about these illusions: Spacial Disorientation.
Capability illusion (The Dunning-Kruger Effect)

The Dunning-Kruger Effect
The Dunning-Kruger effect is a cognitive bias that causes people to overestimate their abilities in a particular area, even when they are incompetent. This can lead to poor decision-making, mistrust, and in some cases, dangerous work conditions. The term was coined in 1999 by Cornell University psychologists David Dunning and Justin Kruger in their paper, “Unskilled and unaware of it: how difficulties in recognizing one's own incompetence lead to inflated self-assessments”. The effect occurs when people lack the expertise to recognize their own shortcomings, and instead evaluate themselves from a limited and subjective perspective.
In the case of the Atlas 3591, I think the First Officer thought he was very good as evidenced by the fact he kept on getting hired. He had excuses for all the failures that led up to his latest job. He might have thought that falsifying his record during interviews was justified because, after all, he was really good.
The Cause (As I see it)
As is common with many NTSB reports, the official probable cause lists what happened (first officer activates TO/GA, gets disoriented, plunges aircraft, captain fails to monitor, FAA doesn't implement Pilot Records Database) but not why it happened. Let's fix that.
- Pilot unions, with the acquiescence of the airlines, have fostered a seniority system that permits aircraft to be piloted with captains with very little time in type. The captain in this accident had only 6 months and 157 hours as PIC in type and less than 4 years time in type including as a first officer. This problem is even more pronounced with the major airlines. See the case study, United Airlines 1722 for an example where the captain only had 300 hours as captain in type and was paired with a first officer with only 120 hours in type.
- Airlines have an economic incentive to get the airplanes in the air no matter the qualifications of those flying them. The minimum standards are in many cases subjective and in a pool of poor performers, the organization may feel compelled to lower their standards to keep aircraft flying.
- The professional pilot "system" encourages poorly performing pilots to keep job hunting until someone hires them without any legal or economic punishment for doing so. Companies willing to hire from the bottom of the pilot pool tend to get more of the same.
In my opinion, if you have an airline captain with fewer than 1,000 hours PIC in type, the first officer should have at least that. Somebody has to be comfortable in the jet. Of course there is a problem: most airlines don't allow the first officer to log any PIC time at all. You end up with captains with inflated PIC hours and first officers with no recorded PIC time at all. Perhaps we should say someone should have at least five years in type. Whatever you do, someone should know what they are doing.
In my opinion, there comes a time where putting fewer aircraft into the sky is the ethical thing to do.
In my opinion, we cannot assume that every pilot in an airline is competent, simply because they've attached the captain title to them. The proposed Pilot Record Database will help, but we have to be willing to use it.
References
(Source material)
Accident Report NTSB/AAR-20/02, Rapid Descent and Crash into Water, Atlas Air Inc. Flight 3591, Boeing 767-375BCF, N1217A, Trinity Bay, Texas, February 23, 2019